최근 글 목록
-
- 2010-2011 새학기 시작: 강...(2)
- rabbit
- 2010
-
- 전쟁과 폭력(2)
- rabbit
- 2010
-
- Neck pain(3)
- rabbit
- 2010
-
- 키보드 또 날렸다... ㅠ.ㅠ(2)
- rabbit
- 2010
-
- “나, 고대 나온 남자야” / ...
- rabbit
- 2010
난 고대도 나오지 않았고, 남자도 아니지만...
같이 읽어볼만한 것 같아서 (근데 누구랑???)
그렇다. 영화 <타짜>의 김혜수가 이대에 대해 가졌던 만큼이나,나도 모교에 대한 자부심이 컸다. 촌놈들이 많이 다니는 학교답게 질박하고 우직한 게 좋았다. 쩨쩨하게 따지지 않고 통 크게 감싸주는 선후배 사이의 정이 푸근했다.
전두환 때다. 말하기 겸연쩍지만, 데모를 하고 감옥을 간 적이 있다. 해가 두 번쯤 바뀌니,공주교도소로 이감을 가란다. “징역살이 어디나 똑같지, 귀찮게….” 투덜거리며 가보니 웬걸, 고대 출신들을 몽땅 모아놓은 게 아닌가. 교도소 당국은 사동 하나를 통째로 비워놓고 방문도 다 따주며 활개치고 살란다. 건달 조직의 두목 조양은씨가 우리들 ‘편의’를 봐주도록 눈감아주기도 했다. 공주지청의 고대 선배 검사는 청요리에 배갈을 잔뜩 먹여, 만취 상태로 교도소에 돌아온 적도 있다. 징역식 과장법을 쓰자면, 비행기 만들어 탈옥하는 것 말고는 다 할 수 있었다.
알고 보니 당시 고대 출신 검찰총장이 고대 총장으로부터 “후배들 신경 좀 써달라”는 부탁을 받고, 화끈하게 선심을 쓴 것이었다. 남들은 비웃겠지만, 그래도 그 살벌한 시기에 정치적 부담을 떠안으면서까지 후배들을 챙겨준 것은 아무래도 ‘미덕’으로 기억된다.
하지만 이명박 정부 들어 고대 선후배 관계가 갈수록 자리를 노린 계산속으로만 흐르는 것 같아 씁쓸하다. 정권 초기 이 대통령 친구 천신일 고대교우회장이 서초동의 고대 출신 검사들을 한자리에 모았단다. “어려운 일 있으면 얘기하라”는 덕담도 빠뜨리지 않았는데, 그게 예삿말로 들리지 않아 참석자들의 표정이 묘했단다. 다들 “줄 한번 타 봐?”라는 유혹을 느꼈을 법하다. 물론 그 대가는 충성이다.
최근 <문화방송> 사태는 그런 ‘주고받기’의 결정판으로 보인다. 엄기영 사장을 쫓아낸 김우룡 방문진 이사장도 고대 출신이고, 빈자리를 꿰차고 들어온 김재철 신임 사장도 고대 출신이다. 이 대통령의 뜻이 반영되었을 터이니 ‘고대의, 고대에 의한, 고대를 위한’ 삼위일체가 완성된 셈이다. 구경꾼들까지 야단법석이다. 고대 문과대교우회가 그 와중에 김우룡 이사장에게 ‘자랑스러운 문과대인상’을 준 것이다.“방송 발전에 앞장섬으로써… 자유·정의·진리의 고대 교시를 온누리에 떨침으로써… 고대의 명예를 드높이셨”다는 게 이유다.
구설은 앞으로도 계속될 모양이다. 당장, 고대 총장을 지낸 어윤대 국가브랜드위원회 위원장이 곧 한국은행 총재나 케이비(KB)금융 회장으로 갈 것이라는 얘기가 파다하다. 특히 최근 한국은행 총재를 인사청문회에 세우는 법안이 무산됐는데, 재산 문제가 께름칙한 어 위원장을 위한 길닦기 성격이 강하단다. 이 작업을 주도한 것으로 알려진 청와대 고위관계자 또한 고대 출신이다. 초등학교 졸업식 노래 3절은 “앞에서 끌어주고 뒤에서 밀며~”로 시작한다. 고대만큼 이 노래의 정신을 잘 구현하는 곳이 어디 있으랴 싶다.
전 총장의 행보가 이러하니, 이기수 현 총장을 보는 시선도 곱지만은 않다. 이 총장이 “대학 등록금이 아주 싼 편”이라고 말했을 때도, 각종 행사장에서 “우리 대통령”을 찾을 때도 그 발언 배경이 파헤쳐진다. 게다가 이 총장 교수실에는 한때 이 대통령과 박근혜 의원이 함께 찍은 낡은 신문 사진이 액자로까지 만들어져 놓여 있었다고 한다. 이 대통령의 맏사위, 박 의원의 올케가 모두 이 총장의 제자라는 걸 은근히 과시하기 위한 ‘장치’라고 해석들을 한다.
고대의 상징은 호랑이다. 입학식 때부터 ‘호랑이는 굶어도 풀을 먹지 않는다’는 얘기를 귀에 딱지가 앉도록 들었다. 그런데 요즘 세태를 보니 호랑이 식성도 많이 변했나 보다.




진보네님의 [블로그에 유투브, 다음 등 동영상 넣기] 에 관련된 글.
내 문의에 대한 답변글이고, 그에 따른 포스팅인데, 아예 전체 다 복사해왔다.
0. ★은 편의상 넣었으니 없다고 생각하세요
1. 유투브 영상에 보면 소스라고 <★object 로 시작하는 거 있죠, URL 말고 그 아래 소스요. 그 소스를 복사하세요.
2. 글쓰기 화면에서 위에 회색 편집기 부분 맨 처음에 "소스"라고 있죠. 소스를 한 번 클릭하시고요, 거기에 1번에서 복사한 내용을 붙여넣으세요(오른쪽 마우스 클릭해서 선택하거나 키보드에서 Ctrl+V).
3. 다시 소스를 누르면 영상이 대충 올라간 게 보입니다.
가끔 영상 아래에 글을 쓰려는데 안 써질 때가 있는데, 그럴 때는 소스부분의 마지막 뒤에 <★br /> 이라고 써주시면 돼요.(별은 빼고)
해보시고 안 되면 다시 문의해 주세요~~
1. 동영상 소스 복사해오기
1-1 유투브
유트브 사이트에 가면 왼편이 영상이고 그 오른편에 올린 사람, 파일 주소 등 여러 정보가 있죠. 그 중
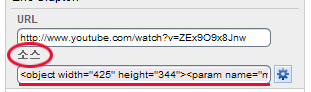
URL 말고 소스 부분의 <★object 로 시작하는 걸 클릭하고 복사하세요. (★은 편의상 넣었으니 없다고 생각하세요)
유투브 사이트가 아니라 블로그나 까페에서 본 동영상을 퍼올 땐

동그란 부분을 누르고 네모난 부분의 <★object 로 시작하는 걸 클릭하고 복사하세요.
진보불로그에는 브라우저에 따라 object로 된 영상은 안 보일 수 있어서, object 말고 embed로 퍼오는 게 더 좋아요. 복사한 내용 중 object가 두 번 나오는데요, 맨앞에 <★object height="344" width="425">(숫자는 다를 수 있음) 라고 써있는 부분과 맨뒤에 라고 써있는 부분을 삭제해 주세요. 이 때 반드시 꺽쇠(< , >)도 삭제하셔야 해요. 자신 없으시면 그냥 놔두시고...;
1-2. 다음 플레이어
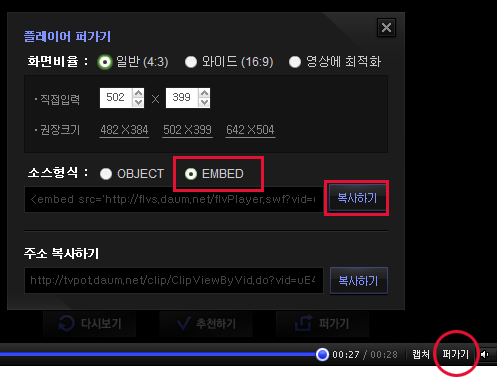
퍼가기 -> EMBED -> 복사하기 하시면 됩니당.
1-3 기타 등등
대체로 퍼가기를 누르고, HTML형식의 소스를 복사해 오는 것은 동일해요. object로 시작되거나 embed로 시작되는 것을 퍼오는 거지요.
2. 블로그에 넣기
"쓰기"를 누르면 글쓰기창 위에 회색 편집기 부분 맨 처음에 "소스"라고 있죠. 소스를 한 번 클릭하시고요, 글쓰기창에 1번에서 복사한 내용을 붙여넣으세요(오른쪽 마우스 클릭해서 선택하거나 키보드에서 Ctrl+V).
3. 다시 소스를 누르면 영상이 올라간 게 보입니다.
가끔 영상 아래에 글을 쓰려는데 안 써질 때가 있는데, 그럴 때는 소스부분의 마지막 뒤에 " <★br />" 이라고 써주시면 돼요.(별은 빼고)
동영상 많이 많이 올리시라능...
New York Time에 실렸다는 글.
누군가가 email로 몇번을 보내서 어쩌다 읽어보게 된 글이다.
가난한 나라 사람들은 미국이나 유럽 사람들이 걸리는 병에 걸려야 그나마 치료약을 얻을 수 있지, 이 나라 사람들이 다 나아버린 경우에는 치료약이 있어도, 제약회사에서 생산을 중단해버려 구할 수가 없다는 얘기
몇 가지 예를 들었는데,
첫번째는 sleeping sickness.
NY Times - March 29, 2006
Talking Points
The Scandal of 'Poor People's Diseases'
By TINA ROSENBERG
It's hard to imagine how a Rwandan woman with AIDS might be considered lucky, but in a way, she is. Effective drugs exist to treat her disease, and their price has dropped by more than 98 percent in the last six years. Research speeds ahead on treatments and vaccines. Although much more needs to be done, the world takes AIDS seriously: rich countries provide money, drug companies have lowered their prices and accepted generic competition, and poor countries like Rwanda are scrambling to provide free treatment to all who need it. None of this is true for people who suffer from malaria, tuberculosis, or a host of other diseases that citizens of rich countries haven't even heard of—like kala azar, sleeping sickness and Chagas disease. Even children with AIDS are out of luck compared to their parents.
All these diseases have been abandoned in some important way. For some, no good treatments exist and there is little attempt to invent them. For others, effective drugs exist, but aren't being made. Or those drugs are so expensive that poor people and poor countries have no hope of buying them. Most of these diseases are easily preventable and completely curable. Saving the lives of their sufferers is much cheaper and easier than treating AIDS. Yet millions of people die of them. Why the difference?
As fatal illnesses go, AIDS is the best one for a poor person to catch because rich people get it, too. The other diseases might as well hang out a sign: "Poor People Only." They offer researchers no profitable market. They have little political constituency. There is no well-connected group of sufferers who stage protests and lobby pharmaceutical companies and Congress to develop better medicines or make existing ones more available. The response to disease is political: the illnesses of invisible people usually stay invisible.
Five years ago, that would have been the end of the story. Today, however, for the best known of these diseases—malaria and tuberculosis—the bleak outlook is starting to change. They are slowly beginning to get the attention, money and research merited by the world's top killers.
People with AIDS all over the world are fortunate to have fellow sufferers in America and Europe. They are even more fortunate that many are middle-class gay men. These men have lots of education, leisure time and income (and usually no kids to spend it on). They are predominantly urban, well-connected and ultra-sophisticated. Their buying power provided pharmaceutical companies with a lucrative market for AIDS drugs. And they lobby. Groups such as ACT UP, which began in the 1980's fighting for the rights of their own members, are now savvy advocates for that woman in rural Rwanda. In poor countries as well, it helps that AIDS strikes all social classes. Brazil would never have become the first poor country to guarantee free AIDS treatment to all who need it without the activism of its many homosexual organizations. For every AIDS victim, though, there are many more suffering from diseases that lack this kind of constituency. Today, contracting a serious disease that affects only poor people is the worst luck of all.
I. How a Beauty Regime Salvaged a Cure for Sleeping Sickness
The story of sleeping sickness is a scandalous illustration of the politics of neglected diseases ~W and of how much wealthy people drive the global medical market. After malaria, sleeping sickness is the most deadly parasitic disease. It is endemic in 36 African countries and is always fatal if it is not treated. The cure used in most places is melarsoprol—an arsenic-based drug so toxic that it collapses each vein into which it is injected and kills between two and eight percent of those who take it. There is another cure, eflornithine, so effective that it is called the "resurrection drug"—it makes people in comas get up and walk.
Eflornithine is an old anticancer drug that turned out to be not very effective against cancer. In the mid-1990's, the company that made the drug stopped making it. The fact that it was extraordinarily effective at treating sleeping sickness didn't matter, because victims of that disease had little money to pay for it. After it stopped production, the company, which is now known as Sanofi-Aventis, licensed the drug to the World Health Organization, which together with the medical charity Doctors Without Borders, searched for another manufacturer. But by 2000, the existing stocks of eflornithine were dwindling and no other manufacturer was interested. It looked as though the miracle cure would disappear. Then lightening struck. Eflornithine reappeared in a six-page ad in Cosmopolitan magazine as the active ingredient in the Bristol- Myers Squibb product, Vaniqa, a new cream that impedes the growth of women's facial hair. Doctors Without Borders, which had just won the Nobel Peace Prize and was launching an initiative to find cures for neglected diseases, seized the opportunity to launch a publicity campaign. Christiane Amanpour went to southern Sudan to report on eflornithine for "60 Minutes."
The predecessor to Sanofi-Aventis, which still controlled the rights to the drug, eventually agreed to donate a five-year supply, plus money for research, surveillance and training of health care workers, in a package totaling $25 million. The donation runs out this year, but there is a good chance it will be renewed. A Bristol-Myers Squibb spokesman inadvertently summed up the plight of sleeping sickness in 2001: "Before Vaniqa came on the scene, there was no reason to make eflornithine at all. Now there's a reason." The market agrees with him. Saving American complexions is a reason. Saving African lives, apparently, is not.
II. Why the Youngest AIDS Victims Suffer Most
AIDS in adults is a global focus of concern. AIDS in children, however, has been ignored.
Last year, 570,000 children died of the disease in poor countries, and 700,000 children became infected with H.I.V. Children should not be getting H.I.V. in the first place. Most of them acquire the virus in the womb, at birth or through breastfeeding. Infection is easily preventable with a drug that costs about a dollar per treatment. In many countries, the drug's producer, Boehringer-Ingelheim, provides it for free. It should be used everywhere in the world. But it is not. When children do become infected with H.I.V., there should be a good antiretroviral treatment for them, as there is with adults. But there isn't. Only about 40,000 children worldwide receive lifesaving antiretroviral drugs to combat AIDS. Children's antiretrovirals are expensive. Even in generic form, they cost three or four times the price of adult drugs. The syrups for young children taste terrible. The cheapest option for older children is to take the generic adult pills, broken by a caregiver into halves or thirds. But this poses a risk of underdosing or overdosing, as a half a pill doesn't necessary contain half its active ingredient.
Since most children with AIDS got the disease from their mothers, most sick kids are being raised by a grandmother or raising themselves. This makes having child-friendly medications even more crucial. One of the most important reasons the AIDS treatment revolution has bypassed kids is that pediatric AIDS is now almost exclusively a third-world disease. Virtually all pregnant women in Europe and North America get AIDS tests. Those who are H.I.V.-positive are either given antiretroviral therapy or a drug to cut mother-to-child transmission of the virus. In 1990, 321 infants were born with H.I.V. in New York City. In 2003, only five were. This is wonderful news for wealthy countries. But it has a deadly side effect: it means there is no more paying market for pediatric AIDS medicines, and no lobbying by those whose children have gotten sick. One result is a dearth of affordable child-friendly drugs. Former President Bill Clinton's foundation has negotiated cheaper prices for generic pediatric AIDS medicines from Cipla, an Indian manufacturer, but this only covers a few drugs.
The disappearance of pediatric AIDS from rich countries harms African children in more subtle ways as well. AIDS doctors and nurses in poor nations need clinical training in how to treat small patients whose doses must change as they grow. But there are few doctors with experience treating pediatric AIDS—they come from places that either don't have the problem, or that don't have the solution. Not much research exists about the long-term effects of antiretroviral drugs on kids. There has been little push to improve diagnostic tests or bring down their price—a serious problem, because the most widely used tests do not work in children under 18 months old.
III. Why One Million Africans a Year Die of Malaria
Malaria used to be common as far north as Canada and Britain. It killed Oliver Cromwell. Shakespeare refers to it, as "ague," in eight of his plays. But today, many Americans don't even realize it is still around. Malaria is all but invisible despite the fact that it is one of the world's top killers, with over a million victims a year in Africa alone. It is the leading cause of death for children under five in Africa. Because rural children don't lobby, malaria is ignored even in Africa. Governments have come to accept a million child deaths as the natural order of things.
Malaria's victims suffer from their invisibility. One way is through lack of money to fight the disease. International organizations and aid agencies talk a lot about malaria. But they have not backed their talk with money. The solutions they push have been things poor people can buy for themselves, because most donors are unwilling to finance more effective measures. All over Africa, a main cure for malaria is chloroquine. The great advantage of chloroquine is that it costs only a few pennies, so even poor African families can buy it. It just has one small problem—in most places it doesn't work. The parasite has become resistant to it. There is a new, effective cure, called artemisinin-based combination therapy. Countries should be switching to it rapidly, but they are not, because it's much more expensive—around $1.40 for an adult cure, 40 cents for a child. That doesn't seem like much to save a life, but it's more than most malaria-stricken families can afford. That means rich-country donors would have to pay. Until recently, they haven't.
Now the United Nations' Global Fund to Fight AIDS, Tuberculosis and Malaria is starting to help countries switch to a malaria cure that actually works. Wealthy nations are also eager to help prevent the spread of malaria—as long as it doesn't cost much. The hot prevention tool today is an insecticide-treated net to hang over a bed. These bed nets are very effective, if people can get them. But people can't, because donors don't want to give them away. Even at the subsidized price of three dollars, the cost is high enough so that people living on a dollar a day do not buy them. One survey asked rural Africans what they would buy if they had the money. A bed net was sixth on the list. The first three items were a radio, a bicycle and, heartbreakingly, a plastic bucket.
Bed net sale programs generally do not work. In contrast, the country of Togo in 2004 gave away bed nets during its national measles vaccination days. Everyone who brought a child to be inoculated got a free bed net, or a voucher for one. Virtually overnight, Togo acquired an effective form of malaria prevention for most of its young children. But this is a solution many donors seem unwilling to finance.
The United States, of course, didn't beat malaria with bed nets. It killed mosquitoes with insecticide—something that African nations also did with much success half a century ago. Today, South Africa and Mozambique have drastically reduced malaria cases with a program to spray the insides of houses with small amounts of insecticide once or twice a year. Why don't other nations do this? Because it requires government financing, and that means rich countries have to pay. So far, they remain reluctant.
The truth is that many malaria victims would be better off if America still had the disease. If malaria still existed in America, we would be attacking it with DDT. In fact, we did exactly that. America sprayed DDT in large quantities on crops and cities. This was extremely irresponsible and did terrible environmental harm. But now we know that DDT can beat malaria without environmental damage, if it is used as it is in South Africa, sprayed in tiny amounts inside houses. DDT, however, is banned in the United States and Europe. That means that Washington has not, until the last few months, financed its use anywhere else and it has blocked the World Health Organization from issuing recommendations to use DDT. American officials maintained it was hypocritical to push an insecticide overseas that is banned at home. Americans are beginning to realize, however, that it is more hypocritical to deny Africa the ability to use responsibly the tools we used irresponsibly to beat malaria. Last year, President Bush announced a new program to fight malaria in Africa that he says will provide an additional $1.2 billion over the next five years. Such promises have a way of drying up, especially when they concern programs with little political constituency. But the program is well-conceived. It will give away bed nets, buy malaria drugs that work and finance indoor spraying. Eight countries in Africa are due to start spraying this year, and three will use DDT as their primary insecticide.
IV. Tuberculosis, Another Overlooked Killer
To many, tuberculosis is a disease of the past, reminiscent of Keats, the Bronte sisters, and a time when it was it was a death sentence all over the world. But it is only the cure that is outdated.
The current cure for TB involves taking a six- to nine-month course of four drugs, the newest of which is 40 years old. The currently used—and not very effective—TB vaccine was invented 80 years ago. The most commonly used diagnostic method is hit-or-miss, and it doesn't work at all on people with AIDS. Until very recently, there was no research designed to solve any of these problems. But while the treatment of TB remains mired in the past, TB is, unfortunately, a disease of the future. Once thought to be disappearing, it has roared back, propelled by AIDS. In sub-Saharan Africa, TB cases are rising at six percent a year. One third of the world lives with the TB bacillus in latent form. When AIDS degrades a person's immune system, it activates TB, which has now become the number one AIDS-related killer. In some parts of Africa, 75 percent of people with AIDS also have TB. And they tend to be the poorest. Sons of presidents get AIDS, too, but they are unlikely to get tuberculosis. That has helped keep the disease invisible even as the numbers soar.
Five years ago, however, something happened. With financing from the Bill and Melinda Gates Foundation, researchers and public health officials created the TB Alliance. It scours universities and corporations for compounds—both existing drugs and brand new ideas—that might have promise against TB. It negotiates rights to these substances, then raises money to develop and test them, and to obtain regulatory approval—the things no drug company is interested in doing. A companion organization is doing the same for TB vaccines, and another one is taking on TB diagnostic tests. As a result, a drug pipeline that once held nothing now has several promising compounds in clinical trials that might allow a faster, less toxic TB cure.
The story of poor people's diseases has not been a happy one, but things are finally beginning to look up. From 1975 to 1999, only 13 new drugs for neglected diseases were invented. Since 2000, however, 63 new compounds have been put into development, including 18 that are in clinical trials. Most of these new compounds are being managed by groups like the TB Alliance, which go by the unwieldy name of public-private partnerships. These groups ~W including the Medicines for Malaria Venture , the Malaria Vaccine Initiative , and the International AIDS Vaccine Initiative ~W are starting to bring real hope to the problem of third world diseases. One World Health is a nonprofit pharmaceutical company that is trying to find cures for illnesses like diarrhea and Chagas disease. Its first product, a cure for a deadly tropical parasite called visceral leishmaniasis, which infects 500,000 people a year, is about to be submitted to India's drug regulatory agency for approval. Doctors Without Borders has its own organization, the Drugs for Neglected Diseases Initiative. The big pharmaceutical companies are also starting to pay more attention. Novartis, AstraZeneca and GlaxoSmithKline have established research labs dedicated to tropical diseases, and many of the largest drug companies are donating medicines. Several companies have programs to work on diseases in specific African countries.
One reason for the surge of interest is AIDS itself. Although many researchers who work on malaria and TB resent the fact that AIDS has hogged most of the attention and financing, the disease has awakened world interest in Africa and poor-country diseases. The pharmaceutical industry has also learned an important lesson with AIDS. Its efforts to maintain high prices and keep out cheap generic drugs—even from poor countries that would not be able to buy brand name medicines—led to worldwide notoriety, and even public comparisons with the tobacco companies. The industry has not reformed. The companies have successfully pushed Washington to negotiate clauses in free trade deals that will make it harder for some of the world's most miserable countries to get generic drugs. But they have begun programs of research and donations of drugs for neglected diseases in part as a way to burnish their image.
The AIDS pandemic has also given birth to the United Nations' Global Fund to Fight AIDS, Tuberculosis and Malaria, which has become a remarkably efficient ongoing source of money, although one hobbled by wealthy governments' stinginess. The partnerships and the pharmaceutical companies can now be assured that someone with money will buy a new AIDS, TB or malaria drug. They may not make a profit, but they won't take a loss. The other reason for the sudden visibility of poor-country diseases is the establishment of the Gates Foundation, which has $5.8 billion in active global health grants at the moment. There is probably not a single major organization working on any kind of vaccine, diagnostic tool, cure or treatment for any poor country disease that does not get much or most of its financing from the Gates Foundation.
When he began his philanthropy in 1994, Bill Gates was looking to locate and fix market failures and get a lot of results for the buck. He certainly has done that. But how many people have died unnecessarily if one person—albeit one very rich person—can stimulate so much progress in reversing a planet's worth of neglect?
Lela Moore contributed research for this article.

최근 댓글 목록